

The Key Message
- What you need to understand
- In the under-eye area, "one problem" almost never explains everything. Usually it's a combination of structure, quality, and light/shadow — which is why a correct diagnosis matters more than any "trendy treatment."
Three Conditions That Can Look Like "Bags Under the Eyes"
Many people say: "I have bags under my eyes." But "bags" is a visual description — not a diagnosis. The under-eye area is one of the most anatomically and aesthetically complex regions of the face: the skin is thin, the tissues are delicate, and the area is heavily influenced by light and shadow, fluid status, collagen quality, cheekbone structure, and facial expression. So the same external appearance can arise from entirely different mechanisms.
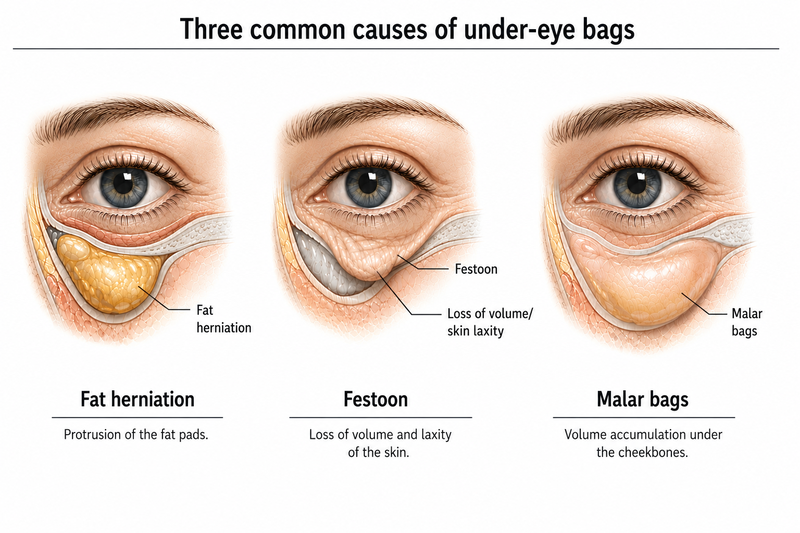
Three particularly common conditions that can look similar at first glance are:
- Lower-eyelid fat herniation (orbital fat herniation) – protrusion of fat from within the eye socket.
- Festoons – a soft fold/pouch along the eyelid–cheek border, sometimes with a fluid component.
- Malar bags / malar edema – swelling in the upper cheek area over the cheekbone.
It's important to understand the differences, because they determine what can be improved by enhancing skin and tissue quality, and what requires a surgical solution (especially when there's significant fat herniation).
The aim of this page is to explain clearly: where each condition "sits," what causes it, how to recognize clinical cues, and what the accepted therapeutic approaches are — including how improving tissue quality (collagen) can help with festoons and malar bags, but does not "treat" significant fat herniation on its own. It also helps preserve a natural, quiet result over time.
Relevant Anatomy: What's Beneath the Skin
The under-eye area is built of thin layers. The small differences between these layers create the differences in appearance:
- Skin – particularly thin, with little subcutaneous fat (compared to the cheek).
- Eyelid muscle (Orbicularis oculi) – a ring-shaped muscle around the eye that affects folds and dynamics.
- Connective tissues and ligaments – create "boundaries" and separations between regions.
- Orbital septum – holds orbital fat in place.
- Orbital fat pads – fat inside the eye socket.
- Midface / upper cheek tissues – soft tissues over the cheekbone, sometimes prone to edema.
Over the years there's a decline in dermal thickness and collagen quality, a change in elastin, and weakening of ligaments. In addition, fluid drainage patterns and subtle inflammatory processes can influence the "softness" of the tissues. That's why in some people there's fluctuation (morning vs. evening), and in others the appearance is more constant.
A practical point: sometimes what bothers people isn't just the "bulge," but specifically the sharp transition between eyelid and cheek. Even a small change in the "transition" can change how the face looks when tired, in a photo, and in strong light.
Fat Herniation: Why "Improving the Skin" Doesn't Make It Disappear
Fat herniation is a condition in which the fat pads inside the eye socket bulge forward. The common cause is weakening of the orbital septum: when the septum "holds" less, the fat pushes forward and creates a bulge near the lash line. This is a true anatomical change — not just swelling.
How does it usually look? A bulge close to the lash line, relatively constant throughout the day, and less affected by posture. When the skin is thinner, the bulge appears more prominent. Sometimes there are "three small furrows" (medial / central / lateral) corresponding to the distribution of the fat pads.
Here we need to be precise: biostimulatory or texture-focused treatments can improve the quality of the surrounding skin (thicker dermis, fewer crepey lines, less translucency), but they don't push orbital fat back in when there's significant herniation. In such cases, the most effective treatment is usually surgical (blepharoplasty) — controlled removal or repositioning of the fat.
Another important point: when there's significant fat herniation, trying to "camouflage" it by adding volume in the wrong area may add mass and worsen the appearance. So the decision whether to even consider volume in this area should be cautious and depend heavily on the diagnosis.
Festoons: A Soft Fold/Pouch Arising from Tissue and Skin
Festoons are soft folds or pouches at the border between the eyelid and the cheek. They differ from fat herniation in that the focus isn't "orbital fat coming out," but a combination of skin laxity, a decline in tissue quality, and sometimes a fluid component.
A common clinical clue: festoons can vary over the course of the day. Many people feel the area is more prominent in the morning, after sleep, after alcohol, during allergy seasons, or after crying / congestion. This variation suggests a fluid component in addition to the tissue fold.
Contrary to common belief, festoons aren't always "a volume problem." Sometimes the issue is that the skin and tissue have lost their internal "scaffolding" (collagen), and so the fold looks sharper. That's why approaches aimed at improving skin and tissue quality may help — particularly when there are crepey lines / thinness / tissue weakness around the fold.
In simple terms: if the skin in the area is thin and fragile, every small bulge "looks like a pouch." When we improve skin quality, the same structure can look less dramatic.
Malar Bags / Malar Edema: When the Swelling Sits on the Cheekbone
Malar bags sit lower than the lower eyelid, over the cheekbone (malar eminence). Sometimes they look like a soft "cushion" on the upper cheek, and sometimes they're more pronounced when smiling. When it's malar edema, the fluid component is more significant, with fluctuation based on time of day, diet, allergies, and congestion.
Why does it look this way? In the upper cheek area there are soft tissues affected by ligaments, fluid drainage, and the quality of the skin above. When the skin is thin and the tissue less stable, any small fluid change looks more prominent. So treatment aimed at improving skin and tissue quality can reduce the "highlighting" of the swelling, even if it doesn't entirely change the deep anatomy.
Many patients describe that malar bags "look worse" when tired, after flights, or during allergy seasons. This doesn't mean the structure has changed — it means the fluid / inflammatory component is emphasizing it.
Quick Comparison Table: Features of Each Condition
| Feature | Fat herniation | Festoons | Malar bags / edema |
|---|---|---|---|
| Location | Close to the lash line | Eyelid–cheek border | Over the cheekbone |
| Fluctuation during the day | Usually low | Sometimes high | Sometimes high |
| Fluid component | Usually not dominant | Can be significant | Sometimes significant |
| What "drives" the appearance | Protruding orbital fat | Skin/tissue + fold | Midface tissues + fluid |
| Main treatment approach | Often surgery | Improving tissue/skin quality | Improving tissue quality + addressing the fluid component |
The table doesn't replace an examination, but it illustrates why "the same bag" can actually be three different problems.
How to Distinguish Between These Conditions: Simple Clinical Cues
There's no substitute for a medical assessment, but there are cues that help you understand what's dominant:
- Location: fat herniation is close to the lash line; festoons at the eyelid–cheek border; malar bags over the cheekbone.
- Fluctuation: if it "comes and goes" (morning / evening) — there's often a fluid component (festoons / malar edema).
- Movement: if the appearance changes during smiling / talking — it's often related to upper cheek (malar) tissues more than to fat herniation.
In addition, light and shadow can be misleading: light from above creates a shadow beneath anatomical edges. Sometimes a "bag" is mostly a shadow created by grooves and sharp transitions between areas. That's why the same person can look "tired" in one camera and less so in another.
In a medical exam we also look at skin quality (thinness, crepey texture, translucency), fat distribution, and how the tissue "sits" relative to the bone and ligaments. That's what allows us to choose a treatment that fits the mechanism.
Why Fillers Sometimes Worsen Festoons / Malar Edema
Fillers can be an excellent tool in the right indications, but in the under-eye area — and especially when festoons or a tendency to edema are present — there's a risk of a puffy appearance. Some materials can draw water and add mass. If the dominant problem is already softness / fluid / a skin fold, adding mass may emphasize the area, deepen a transition line, and sometimes worsen a shadow.
Another point: volume doesn't change collagen quality. It can temporarily alter optics, but doesn't always treat the biological root (thin dermis, texture, tissue quality). So in many cases of festoons / malar bags, it's better to think in terms of restoring tissue quality rather than just "filling."
This doesn't mean filler is always "forbidden" — it means it requires careful matching: who the candidate is, what the dominant issue is, which material, at which plane, and at what dose. When festoons / edema are suspected, it's very often simply not the first tool.
How Improving Skin Quality Can Help: Thickening the Dermis and Strengthening the "Frame"
Skin quality in the under-eye area depends primarily on the dermis — the layer where collagen and elastin reside. Over the years, collagen production declines, its organization changes, and the skin becomes thinner and more fragile. The result: less "scaffolding" support, more crepey lines, and emphasis on borders, folds, and swellings.
When we succeed in improving skin quality gradually (some thickening of the dermis, more uniform texture, less translucency), festoons and malar bags can look less prominent, because the skin "holds" better and the transitions look softer.
Limits matter: this isn't a magic fix, and it doesn't replace surgery for significant fat herniation. But in suitable patients, it can be the difference between a "jumpy" look and a calmer one.
In a regenerative approach, the goal is to encourage gradual repair rather than to "patch over" the problem with immediate volume. Responses are usually cumulative: improved texture, fewer crepey lines, less emphasis on a fold, and sometimes less "reflection" of light off a swollen area.
Treatments That Can Improve Festoons and Malar Bags
When the diagnosis fits (meaning the dominant issue is tissue quality / laxity / edema and not significant fat herniation), there are several approaches aimed at improving collagen structure and skin texture.
PRF Microneedling
Microneedling creates controlled stimulation of the skin, and PRF (Platelet-Rich Fibrin) provides a biological signaling environment that can support healing and gradual repair processes. It's usually delivered in a series, with results appearing gradually over weeks to months. The aim is quality: texture, vitality, and subtle thickening.
Targeted biostimulation (collagen)
When we talk about biostimulation in a delicate area like under the eyes, we mean approaches aimed at supporting dermal repair and reducing "crepiness" and fold emphasis. The principle: improving the tissue, not "adding immediate volume."
Polynucleotides (Polynucleotides / "salmon sperm")
Polynucleotides are a biological approach aimed at improving skin and tissue quality through support for repair processes. The goal isn't "volume," but improving quality: texture, elasticity, and a feeling of "healthier skin" in thin skin. As with many biological treatments, the response is gradual and measured across a series.
Lasers and dermal remodeling
Certain laser technologies can promote dermal remodeling and improve texture. The aim is to "strengthen the scaffolding" of the skin so that the appearance of a fold / swelling becomes less pronounced. In the under-eye area, careful matching is needed to maintain safety.
What about the "fluid component"?
When there's a clear fluid component (edema), it's sometimes also necessary to look at factors that worsen it: allergies / congestion, sleep, alcohol, salty foods, and habits around the eyes (rubbing). This isn't an "aesthetic treatment," but it can greatly influence the outcome and stability.
In most cases, the right plan is a staged plan: first understand the mechanism, then choose one or two approaches that fit, then evaluate the response and adjust.
Realistic Expectations: When Changes Appear and What Counts as Success
One reason for frustration in the under-eye area is the expectation of an immediate change. Treatments aimed at improving skin quality and collagen are generally process-based: the skin needs time to respond, build tissue, and reorganize.
Typically, initial improvement in texture can appear after a few weeks, but more significant improvement tends to accumulate over months — especially when working in a series. So success in this area is sometimes measured in terms of:
- Fewer "crepey lines" and less crinkled skin
- Less emphasis on a fold / sharp transition
- A more even appearance in photos and in strong light
- Gradual, stable improvement (not "volume" that looks good for a week and then disappears)
If the goal is to "completely eliminate" large fat herniation — that's usually not realistic without surgery. But if the goal is to improve tissue quality and reduce the tired appearance caused by folds / thinness / edema, there's much more room for precise regenerative work.
Another important point: the under-eye area is delicate with little margin for error. So "more treatment" doesn't always mean "more result." Sometimes a conservative and precise plan — with follow-up and image comparison in consistent lighting — is better than an aggressive attempt to "close" the problem in one treatment. Precisely a small but consistent improvement in skin quality and collagen structure can be the difference between a natural, fresh appearance and a puffy or uneven one.
Summary: What Can Be Improved and What Requires Surgery
- Significant fat herniation is an anatomical problem of protruding fat — and the effective solution is usually surgical.
- Festoons are related to laxity / tissue quality and sometimes to fluid — and can sometimes be improved by improving skin and collagen quality.
- Malar bags / malar edema are influenced by the upper-cheek tissues and the skin above them — and can sometimes be improved with biostimulatory approaches and texture improvement.
The Key Message: first understand the mechanism, and then choose a treatment that addresses the mechanism — not just the appearance. If you want to know what's dominant in your case (structure, skin quality, or a fluid component), a short medical assessment can sort it out.
More in Sub-Topic Pages
- Why hollows form under the eyes over time
- Dark circles: pigmentation, volume loss, or thin skin
- Festoons, malar bags, and fat herniation — how to tell them apart
- Why under-eye fillers don't always work
- Why tissue quality matters in the under-eye area
- Biostimulatory approaches for delicate under-eye skin
- How lighting and facial structure create a tired appearance
- The Anatomy of the Tear Trough Area